
I’m flabbergasted when people assert that America’s costly and inefficient healthcare system is proof that free markets don’t work.
In hopes of helping them understand what’s really going on, I try to explain to them that an unfettered market involves consumers and producers directly interacting with their own money in an open and competitive environment.
I then explain why that’s not a description of the U.S. system. Not even close. As I noted in Part I, consumers directly finance only 10.5 percent of their healthcare expenses. Everything else involves a third-party payer thanks to government interventions such as Medicare, Medicaid, the healthcare exclusion, the Veterans Administration, etc.
Obamacare then added another layer of intervention to the existing mess. By my rough calculations, that costly boondoggle took the country from having a system that was 68-percent controlled and dictated by government to a system where government dictates and controls 79 percent of the system.
This is very relevant because Republicans in Washington are now trying to “repeal and replace” Obamacare, but they’re confronting a very unpleasant reality. Undoing that legislation won’t create a stable, market-driven healthcare system. Instead, we’d only be back to where we were in 2010– a system where government would still be the dominant player and market forces would be almost totally emasculated.
The only difference is that Republicans would then get blamed for everything that goes wrong in the world of healthcare rather than Obama and the Democrats (and you better believe that’s a big part of the decision-making process on Capitol Hill).
Yes, the GOP plan would save some money, which is laudable, but presumably the main goal is to have a sensible and sustainable healthcare system. And that’s not going to happen unless there’s some effort to somehow unravel the overall mess that’s been created by all the misguided government policies that have accumulated over many decades.
This isn’t a new or brilliant observation. Milton Friedman wrote about how government-controlled healthcare leads to higher costs and lower quality back in 1977, but I can’t find an online version of that article, so let’s look at what he said in a 1978 speech to the Mayo Institute.
I realize that many people won’t have 45 minutes of spare time to watch the entire video, so I’ll also provide some excerpts from a column Friedman wrote back in the early 1990s that makes the same points. He started by observing that bureaucratic systems have ever-rising costs combined with ever-declining output.
…a study by Max Gammon…comparing input and output in the British socialized hospital system…found that input had increased sharply, while output had actually fallen. He was led to enunciate what he called “the theory of bureaucratic displacement.” In his words, in “a bureaucratic system . . . increase in expenditure will be matched by fall in production. . . . Such systems will act rather like `black holes,’ in the economic universe, simultaneously sucking in resources, and shrinking in terms of `emitted production.’” …concern about the rising cost of medical care, and of proposals to do something about it — most involving a further move toward the complete socialization of medicine — reminded me of the Gammon study and led me to investigate whether his law applied to U.S. health care.
Friedman then noted how this bureaucratic rule operated in the United States after the healthcare exclusion was adopted during World War II.
Even a casual glance at figures on input and output in U.S. hospitals indicates that Gammon’s law has been in full operation for U.S. hospitals since the end of World War II… Before 1940, input and output both rose, input somewhat more than output, presumably because of the introduction of more sophisticated and expensive treatment. The cost of hospital care per resident of the U.S., adjusted for inflation, rose from 1929 to 1940 at the rate of 5% per year; the number of occupied beds, at 2.4% a year. Cost per patient day, adjusted for inflation, rose only modestly. The situation was very different after the war. From 1946 to 1989, the number of beds per 1,000 population fell by more than one-half; the occupancy rate, by one-eighth. In sharp contrast, input skyrocketed. Hospital personnel per occupied bed multiplied nearly seven-fold and cost per patient day, adjusted for inflation, an astounding 26-fold.
Friedman then explained that the adoption of Medicare and Medicaid hastened the erosion of market forces.
One major engine of these changes was the enactment of Medicare and Medicaid in 1965. A mild rise in input was turned into a meteoric rise; a mild fall in output, into a rapid decline. …The federal government’s assumption of responsibility for hospital and medical care for the elderly and the poor provided a fresh pool of money, and there was no shortage of takers. Personnel per occupied bed, which had already doubled from 1946 to 1965, more than tripled from that level after 1965. Cost per patient day, which had already more than tripled from 1946 to 1965, multiplied a further eight-fold after 1965. Growing costs, in turn, led to more regulation of hospitals, further increasing administrative expense.
Remember, Friedman wrote this article back in 1991. And the underlying problems have gotten worse since that time.
So what’s the bottom line? Friedman pointed out that the problem is too much government.
The U.S. medical system has become in large part a socialist enterprise. Why should we be any better at socialism than the Soviets?
And he explained that there’s only one genuine solution.
The inefficiency, high cost and inequitable character of our medical system can be fundamentally remedied in only one way: by moving in the other direction, toward re-privatizing medical care.
Some readers may be skeptical. Even though he cited lots of historical evidence, perhaps you’re thinking Friedman’s position is impractical.
So let’s fast forward to 2017 and look at some very concrete data assembled by Mark Perry of the American Enterprise Institute. He looks at medical costs over the past 18 years and compares what’s happened with prices for things that are covered by third-party payer (either government or government-distorted private insurance) and prices for cosmetic procedures that are financed directly by consumers.
As you can see, the relative price of health care generally declines when people are spending their own money and operating in a genuine free market. But when there’s third-party payer, relative prices rise.
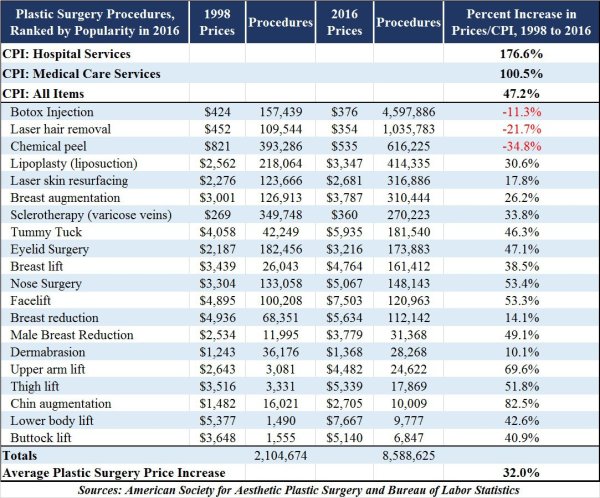
Perry explains the issue very succinctly.
Cosmetic procedures, unlike most medical services, are not usually covered by insurance. Patients paying 100% out-of-pocket for elective cosmetic procedures are cost-conscious, and have strong incentives to shop around and compare prices at the dozens of competing providers in any large city. Providers operate in a very competitive market with transparent pricing and therefore have incentives to provide cosmetic procedures at competitive prices. Those providers are also less burdened and encumbered by the bureaucratic paperwork that is typically involved with the provision of most standard medical care with third-party payments. Because of the price transparency and market competition that characterizes the market for cosmetic procedures, the prices of most cosmetic procedures have fallen in real terms since 1998, and some non-surgical procedures have even fallen in nominal dollars before adjusting for price changes. In all cases, cosmetic procedures have increased in price by far less than the 100.5% increase in the price of medical care services between 1998 and 2016 and the 176.6% increase in hospital services.
In other words, a free market can work in healthcare. And it gives us falling prices and transparency rather than bureaucracy and inefficiency. Maybe when they’ve exhausted all other options, Republicans will decide to give freedom a try.
P.S. If you want to get a flavor for how competition and markets generate better results, watch this Reason TV video and read these stories from Maine and North Carolina.